
Study highlights how spinal cord injury can affect breastfeeding, prompting new clinical guidance to better support mothers.
In Canada, exclusive breastfeeding is recommended for the first six months of a baby’s life, with continued breastfeeding encouraged into the toddler years. Yet, for women with spinal cord injury (SCI), this can present unique physiological and clinical challenges.
For decades, reproductive health in the SCI community has been an understudied area. While more women with SCI are growing their families, gaps in research and clinical guidance persist — sometimes leading to challenges that can begin immediately after giving birth.
One patient partner at the International Collaboration on Repair Discoveries (ICORD) described how her newborn fed well from one breast but struggled with the other. Although her injury affected one side of her body more than the other, neither she nor her care team were certain this was the primary cause.
The quest to better understand how SCI affects breastfeeding set into motion an international research effort led by Vancouver Coastal Health Research Institute (VCHRI) clinician-scientist Dr. Andrei Krassioukov.

In his recent research, Krassioukov found that breastfeeding rates among women with SCI vary widely, ranging from 11 to 100 per cent. Notably, individuals with high-level injuries — affecting the spinal cord closer to the head — were less likely to breastfeed and tended to do so for shorter durations.
These differences are rooted in underlying physiology, he notes. Breastfeeding depends on the “let-down reflex,” where sensory signals from the nipple travel through the spinal cord to the brain, triggering the release of oxytocin and enabling milk ejection. Injuries at or above the thoracic spinal cord can disrupt this pathway.
“If injury is above this level, women may have difficulty breastfeeding or be unable to eject milk, even if it is being produced,” says Dr. Krassioukov.
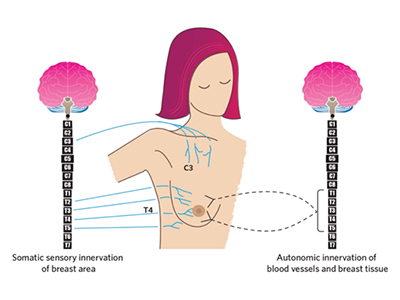
Black lines: autonomic (T1-T5); blue lines: sensory spinal nerves. Milk production requires coordination between these systems.
Breastfeeding also carries the risk of triggering autonomic dysreflexia (AD), a sudden and potentially life-threatening increase in blood pressure caused by stimuli below the point of injury on the spinal cord. Other causes of this reaction include bladder and bowel issues, such as infections or constipation, and factors like tight clothing or skin irritation. Because individuals with SCI may have reduced sensation, the onset of AD can be difficult to detect until it becomes an emergency.
“AD can cause blood pressure to rise so high that a person can have a stroke,” warns Krassioukov.
Research suggests that AD is common in women with injuries at or above what is called the T6 level in the middle region of the thoracic spinal cord, yet awareness of these risks remains low among both families and health care providers.
Lived experience shapes clinical guidance
The research team conducted an international survey involving more than 100 women with SCI. Their findings highlighted not only physiological barriers, but also significant gaps in care.
“Many women told us they did not receive the support they needed during what should be a cherished time,” says Krassioukov.
Some participants described pressure to breastfeed despite complications, while others reported feeling ashamed when it was not possible due to medical reasons.
These experiences reflect a broader issue: many health care providers lack SCI-specific knowledge — particularly in maternal care.
In a national survey of Canadians with SCI, many respondents reported gaps in provider knowledge. For breastfeeding specifically, clinicians may have limited training in how injury level affects milk production, positioning, safety risks and overall care.
To address these limitations, Krassioukov and his team — with support from the Craig H. Neilsen Foundation — developed two complementary resources: clinical practice guidelines for health care providers and a consumer guide for mothers.
The clinical guidelines provide evidence-based recommendations across disciplines, including obstetrics, physiatry, nursing and rehabilitation, with a focus on individualized, team-based care. The consumer guide translates this information into accessible, practical advice to help women understand their options and communicate their needs with care teams.

“Women with spinal cord injury pioneered and shaped the final product of this work.”
The research also emphasizes that some breastfeeding outcomes cannot be predicted based on injury level alone. Instead, clinicians are encouraged to empower mothers to set individualized, realistic goals.
“If you are a care provider who does not have experience with spinal cord injury, ask for help,” says Krassioukov. “And listen to your patients.”
This article uses the terms “breastfeeding” and “mothers” in line with the referenced research. We recognize that some individuals may prefer terms such as “chestfeeding” and “birthing parent."


