Break Wave technology offers a low-barrier treatment option for kidney stone removal that could revolutionize patient care.
The novel Break Wave lithotripsy (BWL) technology offers a game-changing alternative treatment for kidney stones. Discussed in a study led by Vancouver Coastal Health Research Institute researcher Dr. Ben Chew, BWL is a portable and less invasive procedure than the current gold standard treatment, with the potential to enhance access for patients living in remote areas.
“This technology can piggyback onto current ultrasound machines, replacing a diagnostic console with a therapeutic interface,” says Chew.
"BWL is a minimally invasive alternative that can help meet demand for kidney stone treatments across British Columbia.”
Kidney stones are caused by a build-up of salts and minerals in a person’s urine that stick together, forming small, hard deposits. Some people may have a genetic predisposition to developing kidney stones. The condition is also linked to lifestyle and diet, such as not drinking enough water as well as other conditions, such as gout.
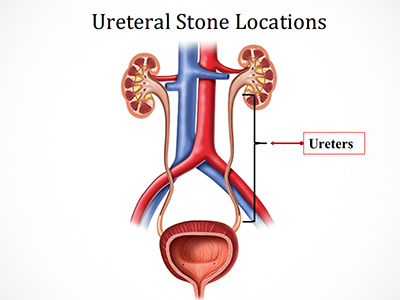
Often painless while in the kidneys, stones that pass from the kidneys to the bladder through narrow tubes called ureters can cause anywhere from mild discomfort to severe pain. Symptoms of kidney stones may also include blood in the urine, nausea, vomiting or painful or frequent urination.
The main approved treatment for kidney stones is extracorporeal shock wave lithotripsy (ESWL), which uses sound wave pulses to break up kidney stones into smaller pieces that are easier and often less painful for the body to pass. While effective, the procedure involves the use of large, expensive equipment, including X-ray imaging technology and an anesthetic, which is only available within hospital settings.
An effective and low-barrier approach to fragment stones in clinic settings
Both BWL and ESWL reduce the size of kidney stones using energy produced by sound waves, represented in megapascals (MPa) of energy. However, ESWL directs a lot more energy at stones — between 40 to 100 MPa — while BWL requires around six to eight MPa to be effective.

“ESWL uses bigger bursts of sound that target the middle of the stone, shattering it from the inside out to form smaller fragments, which is why sedation is required,” explains Chew. “On the other hand, BWL wears away the stone from the outside in to form smaller pieces, theoretically resulting in smaller pieces than ESWL.”
“Patients describe the experience of receiving BWL as a vibrating sensation.”
Patients must fast and complete a bowel prep to cleanse their bowels before an ESWL procedure. Because anesthesia is necessary for the procedure, patients must arrange for someone to pick them up from hospital.
At minimum, a urologist, a nurse, an anesthesiologist and a medical X-ray technologist must be in attendance for ESWL. Additional nursing staff provide post-operative patient care.

By contrast, the non-invasive BWL does not require sedation, fasting or a bowel prep, making it possible for patients to prepare for and travel to and from the clinic or hospital for the procedure in a fraction of time required for ESWL. “We have had patients come to the Stone Centre for a BWL procedure over their lunch hour and then return to work, all on their own,” states Chew.
In their study, published in The Journal of Urology, Chew and international collaborators tested BWL for the first time on 44 kidney stone patient participants. They found the treatment to be an effective and safe means of fragmenting stones in a clinic setting without the use of anesthesia or sedation.
Eighty-eight per cent of patients’ stones were reduced in size, with 70 per cent and 51 per cent of stone fragments measuring less than four millimetres and two millimetres, respectively. Fifty-eight per cent of patients were completely stone-free after receiving the recommended therapeutic treatment of BWL.
While BWL and ESWL are similarly effective at breaking apart stones, BWL is unable to travel through bones or air, whereas ESWL can. As such, Chew anticipates that both BWL and ESWL will be offered moving forwards, with BWL preferred for patients whose stones are not located behind organs or bones.
“The results that we have seen so far are very promising,” Chew says. “BWL technology could play a pivotal role in optimizing patient care access and outcomes, as well as lowering health care costs, including for imaging equipment and staffing resources.”
To further test BWL, Chew and international collaborators are presently conducting a large, multi-site, international Sonomotion stOne comminUtion resoNance ultrasounD (SOUND) Pivotal Trial.


